Ankle Case 9 ED Management
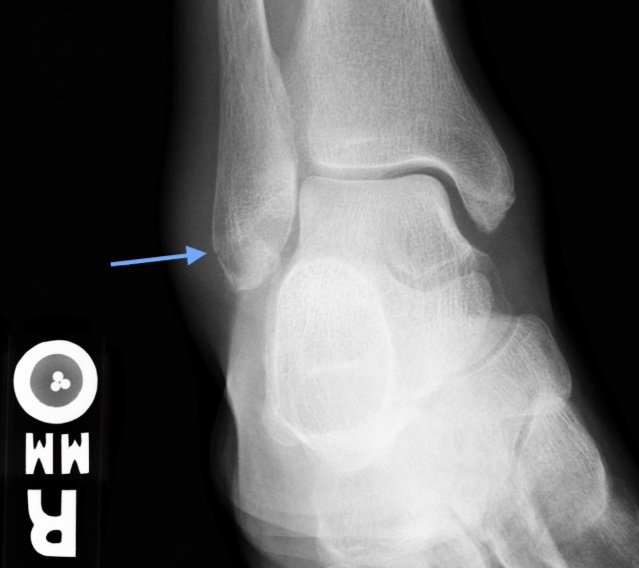
Weber A Fracture
ED Management
When obvious deformity, skin tenting, or neurovascular compromise is present, urgent reduction should be attempted at bedside even prior to obtaining imaging or after a rapidly obtained bedside radiograph. This typically requires parenteral analgesia and possibly sedation. All obvious deformities should be reduced or attempted to be reduced in the ED prior to splinting to achieve as close to anatomic alignment as possible.
Stable fractures (i.e. most Weber A fractures) tend to be managed nonoperatively. For stable Weber A fractures, patients may be placed in a CAM (controlled ankle movement) boot with weight bearing as tolerated and discharged with outpatient orthopedic follow-up in 1-2 weeks to assess for union. If there is any medial tenderness in a Weber A fracture, consider a posterior mold splint and non-weight bearing until follow-up with outpatient orthopedics in about 1 week.